
Right colectomy, or right hemicolectomy, is the surgical removal of the right, or ascending, colon with anastomosis of the remaining ends. It involves division of the ileocolic and right colic arteries as they branch from the superior mesenteric artery (SMA). In 1823, Jean-François Reybard became the first to successfully perform a right hemicolectomy.
Indications
- Benign colon conditions
- Chronic diverticulitis
- Large polyps not amenable to colonoscopic removal
- Large bowel obstruction
- Inflammatory bowel disease
- Uncontrolled bleeding
- Colon cancer
Contraindications
Preoperative Considerations
- Lesion should be tattooed for patients with polyps and occult neoplasms
- Mechanical bowel prep
- Prophylactic antibiotics
Risks
- Conversion to open
- Colostomy
Relevant Anatomy
- Large bowel = colon + rectum; 150 cm in length (roughly 5 feet)
- Covered with peritoneum; no mesentery
- Cecum
- Thinner wall and larger diameter compared to the rest of the colon
- Most likely location to perforate in presence of large bowel obstruction
- Risk of ischemic necrosis and perforation increases with diameter > 12 cm
- Ileocecal valve
- Where terminal ileum empties into cecum
- Thickened, nipple-shaped invagination containing circular muscle
- Appendix
- Extends from cecum 3 cm below ileocecal valve
- Blind-ending elongated tube 8 – 10 cm in length
- Ascending colon
- Begins at ileocecal junction and continues to hepatic flexure
- 15 cm in length (0.5 feet)
- Covered with peritoneum anteriorly and laterally
- Fixed against retroperitoneum by fascia of Toldt posteriorly
- Best mobilized along lateral peritoneal reflection by incising “white line of Toldt”
- Transverse colon
- 45 cm in length (roughly 1.5 feet)
- Covered by visceral peritoneum
- Greater omentum is attached at superior aspect; lifting upward with downward traction will reveal an avascular plane adjacent to the colon (most easily identified close to midline)
- Descending colon
- Begins at splenic flexure (where intestine loses its mesentery) to the sigmoid colon
- Splenic flexure
- Where transverse colon is flexed downward
- Suspended by four mainly avascular ligaments
- Phrenicocolic ligament
- Splenocolic ligament
- Renocolic ligament
- Pancreaticocolic ligament
- Sigmoid colon
- Begins at or below level of iliac crest where colon becomes completely intraperitoneal again
- Thicker and more mobile compared to descending colon
- When mobilizing, the mesenteric fold is the surgical landmark for underlying left ureter
- Ends at rectosigmoid junction (where colonic taenia confluence for form complete longitudinal muscle layer, and colon loses its mesentery)
- Splenic flexure
- 25 cm in length (0.82 feet)
- Commonly dissected along the line of Toldt from below and then enter lesser sac by lifting omentum above transverse colon
- Lesser sac (lesser peritoneal sac, omental bursa)
- Potential space that exists within the abdomen between the stomach and the pancreas
- Formed by greater and lesser omentum
- Lesser sac (lesser peritoneal sac, omental bursa)
- Smaller in diameter than ascending colon
- Begins at splenic flexure (where intestine loses its mesentery) to the sigmoid colon
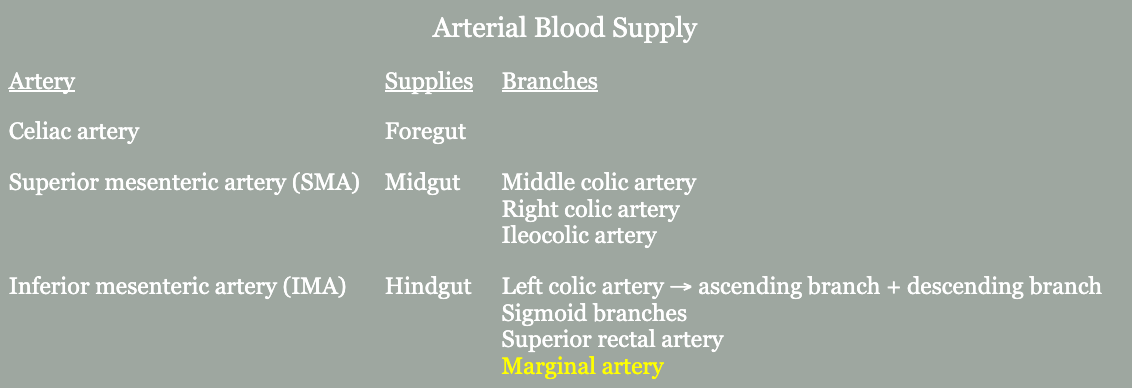
- Meandering mesenteric artery (arc of Riolan, Moskowitz artery)
- Thick collateral vessel that courses closely to the base of the mesentery
- Connects SMA or middle colic artery to the IMA or left colic artery
- Presence suggests occlusion of one of the major mesenteric arteries

Surgical Technique
- Patient is placed in the modified lithotomy position with legs in stirrups. The skin is prepped and draped in the usual sterile fashion.
- Access to the peritoneal cavity is achieved under direct visualization. An incision is made in the umbilicus and a 10-mm port is inserted. The abdomen is insufflated to 15 mmHg. Three additional ports, a 10-mm trocar to the left of midline in LLQ with 5-mm trocars in LUQ and RLQ.
- The right colon is mobilized in a lateral to medial approach, beginning at the cecum. The patient is placed in Trendelenburg and the cecum is grasped and retracted anteromedially. An incision is made in the peritoneal reflexion close to the lateral wall of the bowel at the tip of the cecum. The assistant grasps the ascending colon and retracts it medial and cephalad in order to allow the incision of the peritoneum to be extended upward towards the hepatic flexure. Care should be taken to avoid ureteral injuries. The duodenum may be visualized while approaching the hepatic flexure and should be protected.
- To mobilize the hepatic flexure, the patient is placed in the reverse Trendelenburg position. The hepatic flexure is retracted inferomedially and an ultrasonic device is used to divide the peritoneal attachments. The proximal transverse colon is mobilized next by dividing the omental attachments along the line of dissection. The assistant grasps the omentum and retracts it upward to allow the surgeon to grasp the mesenteric side of the transverse colon and put tension on the omental attachments. The omental attachments are divided with ultrasonic shears or electrocautery. Division of the gastrocolic ligament is often necessary to completely mobilize the hepatic flexure from the liver.
- The mesentery is divided by multiple steps. The ileocolic vessels are grasped and retracted toward the anterior abdominal wall. The peritoneum overlying the mesentery is incised beneath the ileocolic vessels to create a window. For malignancy, this should be near the root of the mesentery. The cecum is grasped and retracted laterally to elevate the ileocolic vessels, which are then skeletonized and divided with the linear laparoscopic stapler with 2.5-mm staples or clips. Dissection is carried toward the hepatic flexure and the stapling process is repeated until the mesentery is divided. Dissection is continued to and including the right branch of the middle colic artery.
- After complete mobilization, the specimen is removed through a port hole, which often needs to be enlarged. The right lower quadrant port can be utilized for this. Traditionally, an infraumbilical or umbilical port site, or an additional suprapubic incision has been for this step. However, herniation is common at the umbilicus and an additional incision can be avoided by elongating an incision that already needs to be made. A plastic wound protector is used for this step.
- The terminal ileum and colon are exteriorized through the RLQ opening. The proximal and distal margins of the specimen are divided using a linear stapler (3.5 mm staples). Larger staples may be needed depending on bowel thickness. A side-to-side hand-sewn or stapled anastomosis may be performed. To perform a side-to-side stapled anastomosis, stay sutures are placed to secure the two antimesenteric walls of the ileum and colon. An enterotomy is made by excising a small portion of the staple line along the ileum and transverse colon to introduce the stapling divide. The linear stapler is then introduced and closed. The posterior aspect of the bowel is examined to be sure no mesentery is included in the closed stapler and once this is ensured, the stapler is discharged and the anastomosis is created. THrough the enterotomy, the staple line is inspected for bleeding and any points are sutured with 3-0 silk figure-of-eight sutures. Once hemostasis is achieved, the enterotomy is closed with a stapler. The mesenteric defect is closed and the bowel is returned to the peritoneal cavity.
- The incision used to exteriorize the bowel and complete the anastomosis is closed and any port sites greater than 5 mm are closed with suture as well.
Postoperative Complications
- Anastomotic leak
- Ureteric injury
- Bleeding
- Infection
- Damage to surrounding structures