
Inguinal hernias are a type of hernia that occurs in the area of the groin, the area between the lower part of the abdomen and thigh, and pass through the inguinal canal. Guy de Chauliac was the first surgeon to differentiate between umbilical and inguinal hernias. The first strangulated hernia was described in 1470 by Bartolomeo Montagnana.
Etiology
- Indirect: incomplete obliteration of the processus vaginalis
- Direct: weak transversalis fascia
Epidemiology
- Increase with age
History
- Pain/discomfort in area of hernia
- Worse with physical activity or coughing
- ± Burning or pinching sensation
- May radiate into scrotum or leg
- Asymptomatic in ⅓ of patients
Physical Exam
- Bulge in the inguinal region, increase in size with increased intra-abdominal pressure (cough, Valsalva, etc.), exam done on both sides while patient is standing
- Indirect: bulge moving lateral to medial in the inguinal canal
- Direct: budge progressing from deep to superficial through the inguinal floor
Imaging
- US can aid in diagnosis, especially if patient has a bulge of the groin not demonstrated on exam; conducted with Valsalva to increase intra-abdominal pressure
Treatment
- Asymptomatic patients → nonoperative, watchful waiting
- Symptomatic patients → surgery
- Anterior repairs
- Tissue repairs
- Tension-free anterior inguinal hernia repair
- Preperitoneal repair
Relevant Information
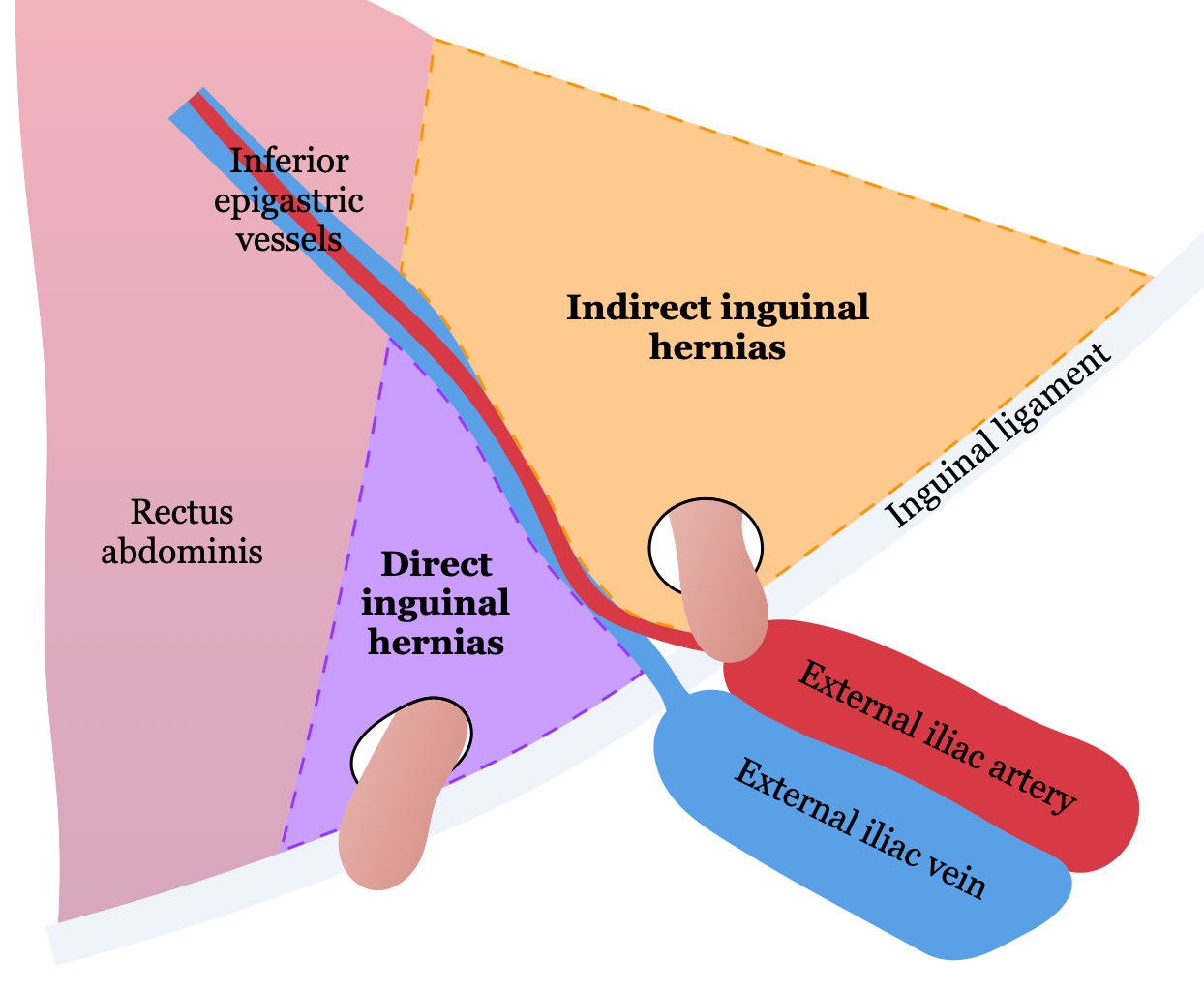
- Hesselbach’s triangle is triangle formed by
- Epigastric vessels
- Inguinal ligament
- Lateral border of rectus sheath

- Types of hernias
- Inguinal: protrusion of intraabdominal contents (usually fat) through the inguinal canal
- Indirect
- Most common type of hernia
- Most common hernia in women
- Protrudes from the internal inguinal ring obliquely toward the external inguinal ring into the scrotum and is lateral to the inferior epigastric vessels
- Direct
- Protrudes outward and forward and is medial to the internal inguinal ring and inferior epigastric vessels
- Littre’s: inguinal hernia with a Meckel’s diverticulum in the hernia sac
- Indirect
- Ventral (abdominal): protrusion of intraabdominal contents through congenital or acquired defect in the abdominal wall
- Incisional: protrusion through previous surgical incision
- Umbilical: protrusion through the umbilicus
- Femoral
- Women more likely to get than men
- Intraabdominal contents herniate into femoral canal through femoral ring, below the inguinal ligament
- Hiatal: protrusion of any abdominal structure into thoracic cavity through lax diaphragmatic esophageal hiatus
- Internal: protrusion of visceral contents through congenital or acquired defect in peritoneum or mesentery within the abdominal cavity
- Pantaloon: when both indirect and direct hernias are seen at the same time
- Richter: protrusion of only a portion of the bowel circumference through a defect
- Spigelian: protrusion in the anterior abdominal wall adjacent to the semilunar line through a slit-like defect; almost all occur at or below the arcuate line
- Littre: hernia involving Meckel’s diverticulum
- Amyand: when the appendix is trapped within an inguinal hernia
- Parastomal: protrusion to side of stoma
- Acquired diaphragmatic: protrusion of intra-abdominal contents through abnormal opening in diaphragm
- Obturator: protrusion through obturator canal (formed by union of pubic bone and ischium)
- Lumbar: protrusion in lumbar region of posterior abdominal wall
- Interparietal: protrusion between layers of the abdominal wall
- Sciatic: protrusion through greater sciatic foramen
- Perineal: protrusion through pelvic diaphragm
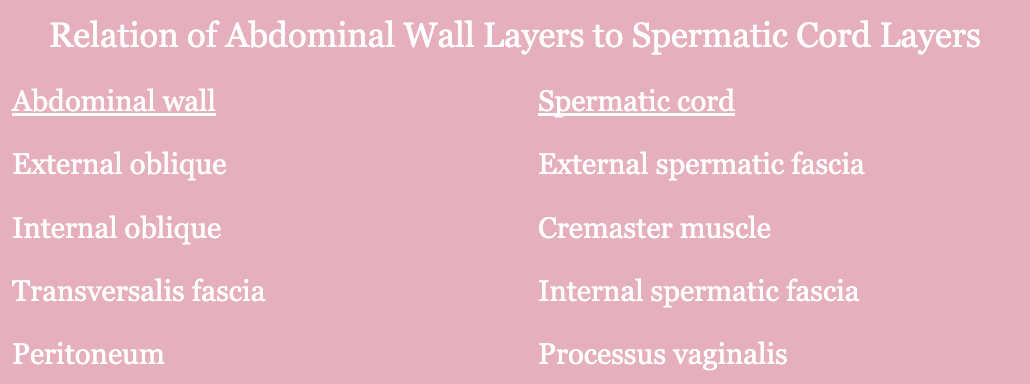
- Cremaster muscle is derived from internal oblique muscle
- Inguinal ligament is derived from external oblique muscle
- Ilioinguinal nerve travels with the spermatic cord
- Structures in the spermatic cord
- Cremasteric muscle fibers
- Vas deferens
- Testicular artery
- Testicular pampiniform venous plexus
- ± Hernia sac
- Within the spermatic cord, the vas lies medial to the testicular vessels
- Cutting the ilioinguinal nerve leads to loss of sensation to the medial aspect of the inner thigh and scrotum/labia and loss of cremasteric reflex
Complications
- Strangulation
- When blood supply to a hernia is reduced or cut off due to compression of blood vessels
- Most strangulated hernias are indirect, but femoral hernias have the highest rate of strangulation of all hernias
- Incarceration: intestines becomes trapped in the hernia sac
- Hernia recurrence
Classifications
- Nyhus classification
- The European Hernia Society Groin Hernia Classification
Differential Diagnoses
- Hydrocele
- Varicocele
- Ectopic testis
- Epididymitis
- Testicular torsion
- Lipoma
- Hematoma
- Sebaceous cyst
- Lymphoma
- Metastatic neoplasm
- Femoral hernia