
Fasciotomy is the surgical incision of the fascia to release the intracompartmental pressure as a result of compartment syndrome. Compartment syndrome was first described in 1881 by the German surgeon Richard von Volkmann.
Indications
- Lower extremity compartment syndrome (intracompartmental pressure > 30 mmHg, delta pressure ≤ 30 mmHg, normal compartment pressure < 10 mmHg)
Preoperative Considerations
- Hemodynamic stability
- Fluid and electrolytes
- Preoperative antibiotics
Relevant Anatomy
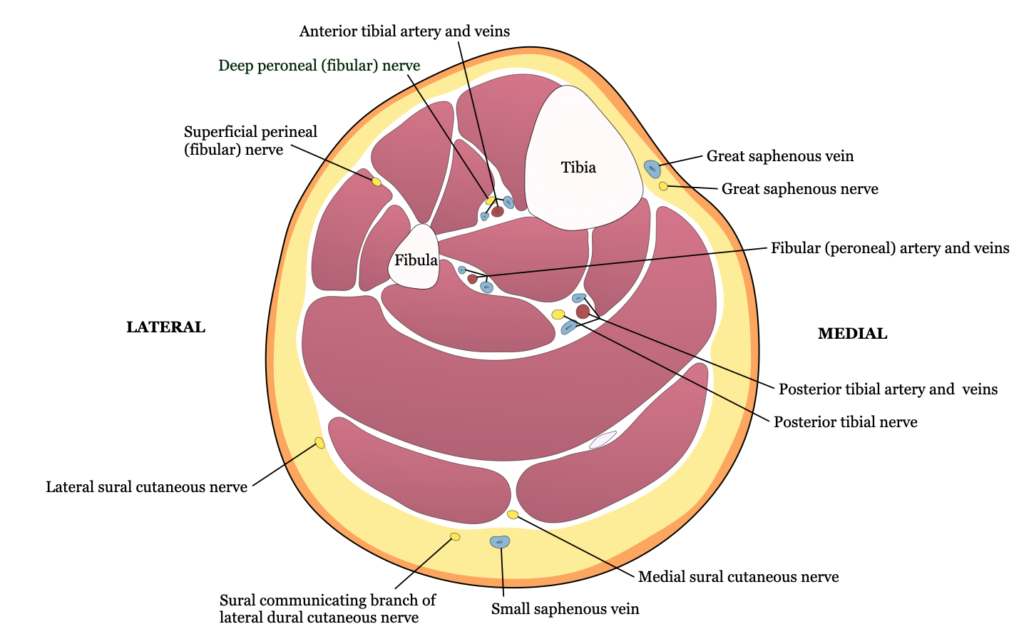
- Superficial branch of the peroneal nerve: lies adjacent to the intermuscular septum between anterior and lateral compartments
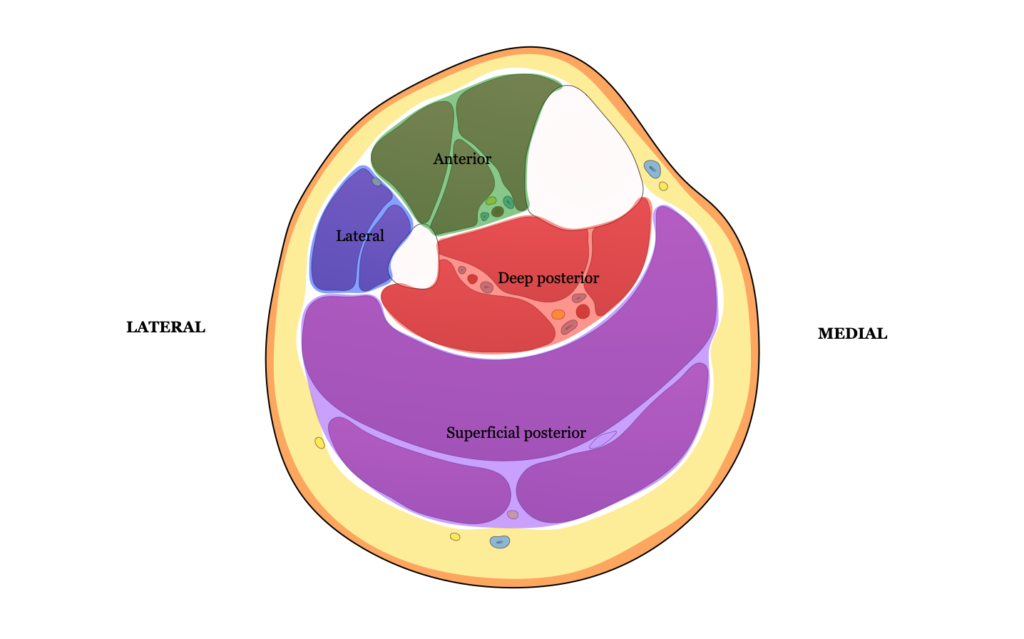
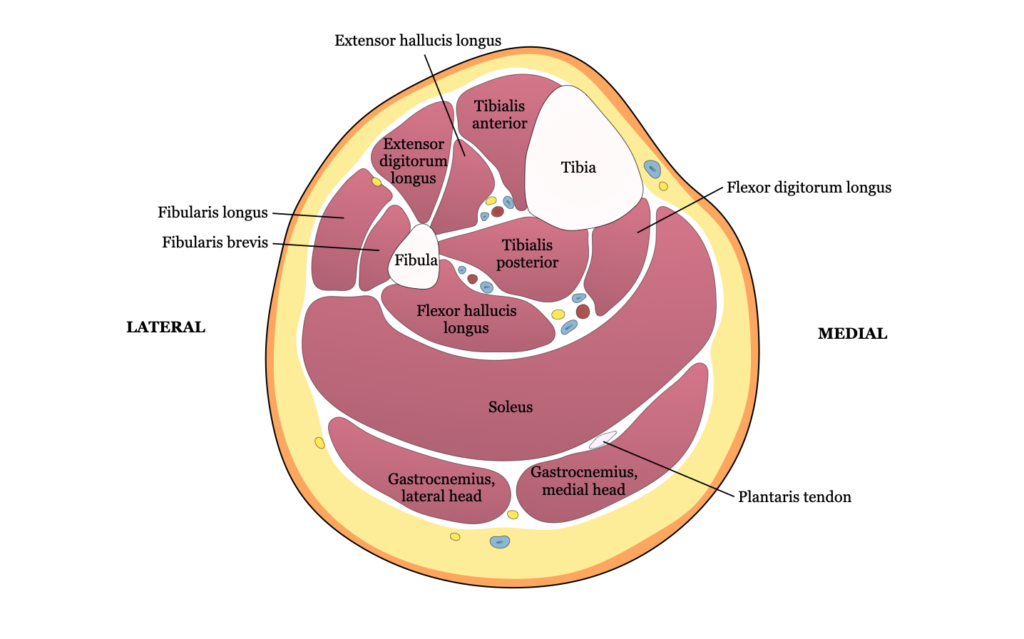
- Compartments of the leg
- Anterior → most common location for compartment syndrome
- Tibialis anterior
- Peroneus tertius
- Extensor hallucis longus
- Extensor digitorum longus
- Lateral
- Peroneus longus
- Peroneus tertius
- Superficial posterior
- Gastrocnemius
- Soleus
- Plantaris
- Deep posterior
- Tibialis posterior
- Popliteus
- Flexor hallucis longus
- Flexor digitorum longus
- Anterior → most common location for compartment syndrome
Relevant Information
- Compartment syndrome is most likely to occur in the lower extremity, likely as a result of ischemia or restoration of flow after a period of ischemia
- Special attention should be given to patients with open fractures as these patients are still at risk for compartment syndrome
Surgical Technique
- The entire leg is prepped and draped in the usual sterile fashion. The entirety of the compartment fasciotomy can be accomplished through two incisions, one incision over the medial calf and another incision lateral to the anterior tibia.
- A longitudinal incision is made over the medial calf, 1 cm posterior to the posterior edge of the tibia. A similar incision is made through the posterior compartment fascia (superficial posterior compartment) through the same skin incision. The gastrocnemius-soleus muscle complex is taken down from its attachments to the tibia (deep posterior compartment).
- Another incision is made several centimeters lateral to the anterior tibia and extended for 10 cm. A similar incision is made through the anterior compartment fascia (anterior compartment), with care given to avoid underlying muscle and bleeding. The tip of Metzenbaum scissors are inserted into the edge of the fascial incision proximally and distally and advanced under the skin to complete the fasciotomy. The lateral compartment is incised in a similar fashion through the same incision.
- Legs are dressed with wet-to-dry dressings.
Postoperative Considerations
- Legs are assessed daily for ability to close either primarily or for alternate management
Postoperative Complications
- Infection
- Bleeding
- Nerve injury