
Appendicitis refers to inflammation of the appendix. The first appendectomy was completed by Claudius Amyand in 1735 when he operated on an 11-year-old male for a strangulated inguinal hernia and discovered the appendix in the hernial sac. The first intentional appendectomy was performed by Lawson Tait in 1880.
Pathophysiology
- Luminal obstruction from various etiologies
- Luminal obstruction leads to increased intraluminal pressure which decreases venous outflow causing lymphatic congestion resulting in tissue ischemia, inflammation, eventual necrosis, and perforation
- Intraluminal bacteria translocate beyond mucosa and potentiate the inflammatory process causing phlegmon or inflammatory mass
Epidemiology
- Peak incidence 10-30 years old
Presentation
- Periumbilical abdominal pain that migrates to RLQ pain
- Anorexia
- Nausea, vomiting
- Fever, tachycardia
- Rigidity → if present, points towards perforation (usually occurs 24 hours after symptom onset)
- McBurney point: ⅓ distance from right ASIS to umbilicus
- Psoas sign: pain with right hip extension
- Secondary to peritoneal irritation
- Specificity 95%, sensitivity 16%
- Does This Patient Have Appendicitis? (JAMA 1996)
- Rovsing sign: RLQ pain with palpation of LLQ
- Due to peritoneal stretch and irritation from contralateral abdominal pressure
- No study completed to demonstrate sensitivity or specificity
- Obturator sign: RLQ pain with right hip internal rotation
- No study completed to demonstrate sensitivity or specificity
- Dunphy sign: RLQ pain with coughing
Workup
- Leukocytosis
- Sensitivity 76%, specificity 52%
- Not highly predictive – absence doesn’t exclude appendicitis
- Pregnancy test should be obtained to rule out ectopic pregnancy
- CT w IV contrast
- Most commonly used; effective and accurate
- Thickened, inflamed appendix with surrounding “stranding” indicative of inflammation, >7 mm in diameter, mural enhancement or “target sign”
- Sensitivity 76-100%, specificity 83-100% (Systematic Review: Computed Tomography and Ultrasonography to Detect Acute Appendicitis in Adults and Adolescents)
- RLQ US
- May have greater utility in pediatric or pregnant patients to avoid radiation
- Success of study depends greatly on skill of the sonographer
- Appendix diameter >6 mm, periappendiceal fat with echogenic enhancement, fluid within RLQ
- Sensitivity 86%, specificity 81% (Systematic Review: Computed Tomography and Ultrasonography to Detect Acute Appendicitis in Adults and Adolescents)
- MRI wo contrast
- Reserved for pregnant patients or second-line imaging when RLQ US is inconclusive
- Appendix dilation >7 mm, thickening >2 mm, presence of inflammation
- Cons: higher cost, motion artifact
Treatment
- Nonoperative management
- CODA trial (2021) compared nonoperative management of appendicitis to appendectomy by looking at >1500 patients
- Appendicolith is 3x more likely to require appendectomy at 48 hours
- Nonoperative management can be presented as alternative to appendectomy but patients must understand risk of recurrent symptoms, future hospitalization, and possible failure to diagnose appendiceal neoplasm
- Concluded that nonoperative management with antibiotics were noninferior to appendectomy. Roughly 30% of patients will undergo appendectomy in 90 days. Patients with appendicolith are higher risk of need for appendectomy compared to patients without appendicolith.
- APPAC III trial
- CODA trial (2021) compared nonoperative management of appendicitis to appendectomy by looking at >1500 patients
- Appendectomy
- Avoid delay >6 hours if possible
- Laparoscopic or open
Relevant Information
- Appendix orientation
- Retrocecal (65%)
- Pelvic (31%)
- Subcecal (2.3%)
- Preileal (1.0%)
- Retroileal (0.4%)
- Fold of Treves
- Bloodless fold; no sizable blood vessels
- Peritoneal structure that extends from the antimesenteric border of the terminal ileum to the base of the appendix, or anterior surface of the mesoappendix, or both
- Can aid in the recognition of the ileocecal region and base of the appendix
Complications
- Perforation: can lead to sepsis, increased risk with prolonged duration of symptoms; rigidity will be present upon physical exam
Scoring Systems
- No signs or symptoms have been shown to be uniquely predictive of appendicitis, so scoring systems have been developed to help with clinical diagnosis
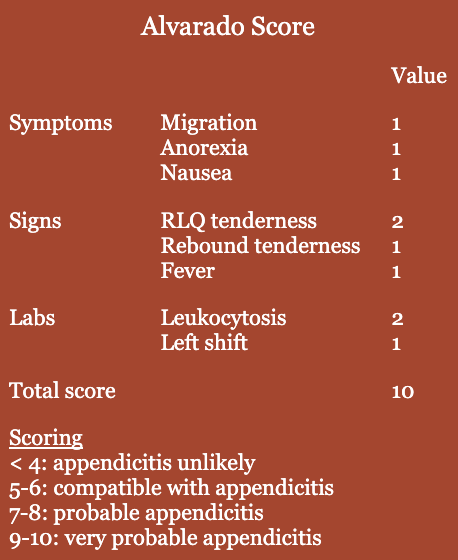
- Alvarado scoring
- 8-item clinical and laboratory variables
- Scoring < 4 useful in excluding appendicitis; higher score lacks specificity
- Most widely used and acceptable
- Pediatric Appendicitis Score (PAS)
- Appendicitis Inflammatory Response Score (AIRS)
Differential Diagnoses
- Crohn ileitis
- Mesenteric adenitis
- Intussusception
- Meckel diverticulum
- Ectopic pregnancy
- Testicular torsion
- Ovarian torsion
- Kidney stones
- Gastroenteritis
- Pelvic inflammatory disease
- Endometriosis
- Renal colic
- Irritable bowel disease