In 1867, four case reports by Rokitansky described carcinoma of the appendix. However, microscopic diagnosis was not provided. The first microscopic confirmed case was in 1882 by Beger. In 1951, G.N. Weiss and A. J Hertzog reported that carcinoid tumors often occur at the tip of the appendix and are seen in about 1/500 appendectomies.
Epidemiology
- Male predominance
- Average age of 60 years old
- Rare (1 per 1,000,000 population)
- 1% of all neoplasms of intestinal tract
Pathophysiology
- Develop via adenoma-to-carcinoma sequence like colorectal adenocarcinomas
- Mutations in KRAS oncogene
Subtypes
- Epithelial
- Mucinous → proliferation of mucin-containing cells
- Mucinous adenocarcinoma
- Infiltrating invasion into at least the submucosa
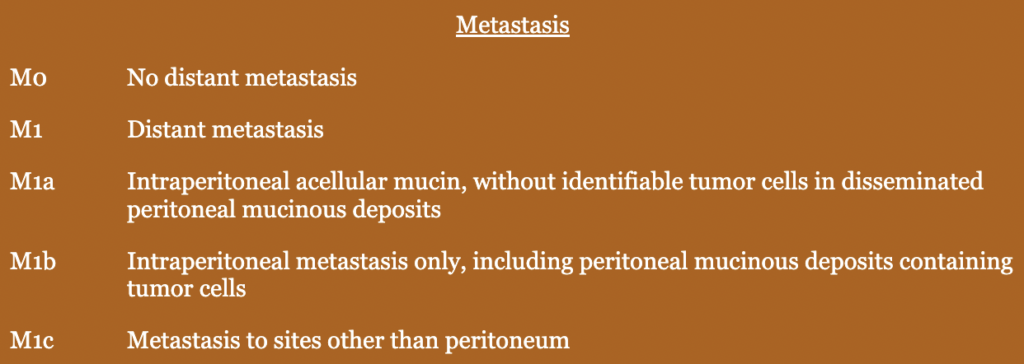
- Most common source of pseudomyxoma peritonei
- Low-grade appendiceal mucinous neoplasms (LAMNs)
- Earliest form of mucinous tumors
- Not inherently malignant
- Mucin-containing cells confined to epithelium and muscularis mucosae
- High-grade appendiceal mucinous neoplasms (HAMNs)
- Higher-grade atypical cells
- Don’t have infiltrative invasion
- Mucinous adenocarcinoma
- Nonmucinous adenocarcinoma
- Adenocarcinoma (colorectal type)
- ⅓ of primary appendiceal cancers
- Slight male predominance
- High rate of lymph node metastasis (highest risk compared to mucinous as well)
- Goblet cell carcinoma
- Arise from intestinal crypt base stem cells
- Tumor composed of goblet-like mucinous cells, neuroendocrine, and Paneth cells
- Behave more like adenocarcinomas as opposed to neuroendocrine
- Adenocarcinoma (colorectal type)
- Note: presence of signet rings is associated with more aggressive cancer and can be found in both mucinous and nonmucinous adenocarcinoma
- Mucinous → proliferation of mucin-containing cells
- Nonepithelial
- Neuroendocrine tumors
- Previously known as “carcinoid tumor” → tumors that metastasize to the liver can cause carcinoid syndrome and present with symptoms such as flushing, diarrhea, bronchoconstriction, and valvular heart disease
- Most common appendiceal neoplasm, and most common site for carcinoid tumor
- Monitored for recurrence every 6-12 months with biochemical (e.g., 5-HIAA) and imaging (e.g., CT, MRI)
- Lymphoma
- Sarcoma
- Gastrointestinal stromal tumors
- Mesenchymal tumors
- Neuroendocrine tumors
- Signet cells on histology is associated with more aggressive cancer. Can be present in mucinous and nonmucinous adenocarcinoma.
Presentation
- Acute appendicitis
- RLQ pain
- Fever
- Nausea
- Most are identified after appendectomy
- Can be found incidentally on colonoscopy or imaging obtained for other reasons
Surgery
- Indications
- Abnormal appearing appendix during exploration
- Appendicitis (2% of all appendectomy specimens harbor an appendiceal neoplasm)
- Known or suspected appendiceal carcinoma (e.g., biopsy-proven adenocarcinoma, obvious adenopathy) → prepare for right colectomy
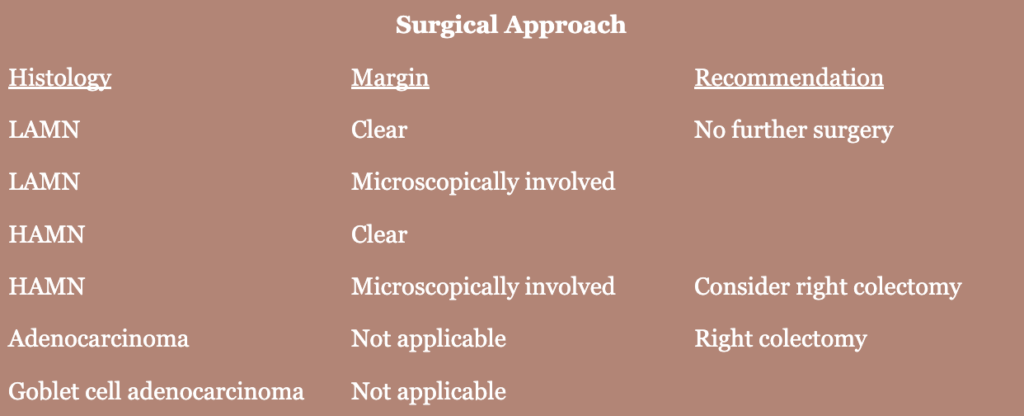
- Surgical approach depends on pathology and clinical findings
- Preoperative planning
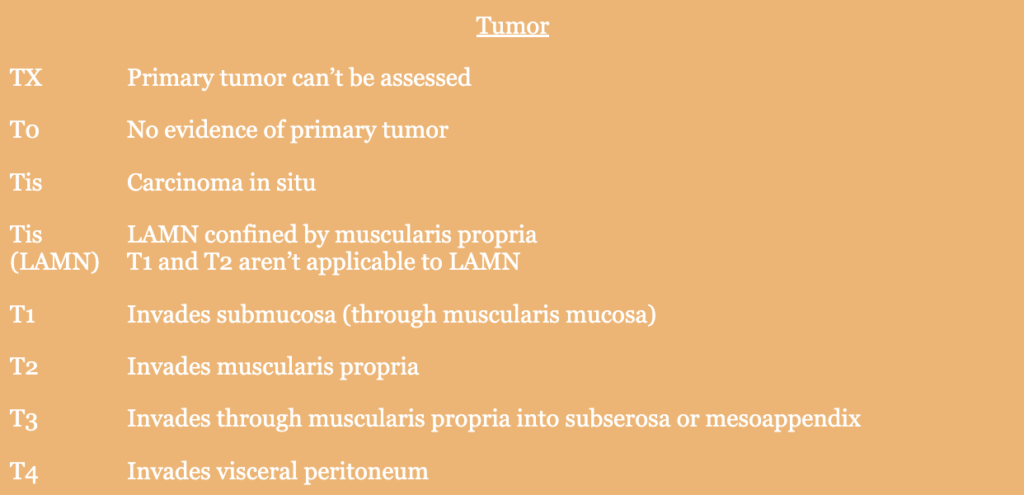
- Staging should be completed if surgery is being completed for a known diagnosis of mucinous neoplasm
- CT chest, abdomen, pelvis
- Full colonoscopy (evaluate for synchronous lesions)
- No evidence to support, but CEA, CA 19-9, CA-125 often elevated and sometimes followed postoperatively as surveillance
- Complete mechanical and antibiotic bowel prep if right colectomy is planned
- Staging should be completed if surgery is being completed for a known diagnosis of mucinous neoplasm
- Technique
- Oncologic principles
- Gentle tissue handling
- Adequate lymph node harvest
- Negative margins
- Avoid rupture or spillage of tumor as it can lead to pseudomyxoma peritonei
- Indications for right hemicolectomy
- Nonmucinous adenocarcinoma
- Due to high rate of lymph node metastasis with appendiceal adenocarcinoma
- Risk is highest for colorectal-type adenocarcinoma compared to mucinous
- Mucinous adenocarcinoma if
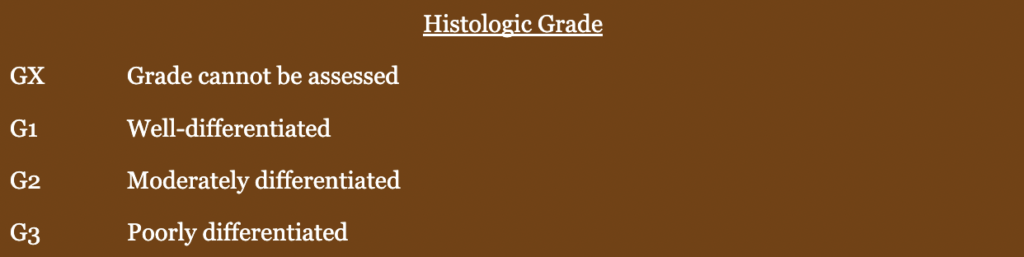
- Moderate to poor differentiation
- Not completely resected
- Ruptured
- Carcinoid tumor
- Consider right hemicolectomy if tumor if positive margin at base of appendix for HAMN
- Neuroendocrine tumor >2 cm in size → may perform right colectomy in neuroendocrine tumor 1-2 cm in size depending on patient presentation and tumor characteristics
- Nonmucinous adenocarcinoma
- Oncologic principles
- Multimodal therapy
- LAMN → no adjuvant therapy
- HAMN → no adjuvant therapy
- High risk tumors → recommend 5-FU-based adjuvant chemotherapy
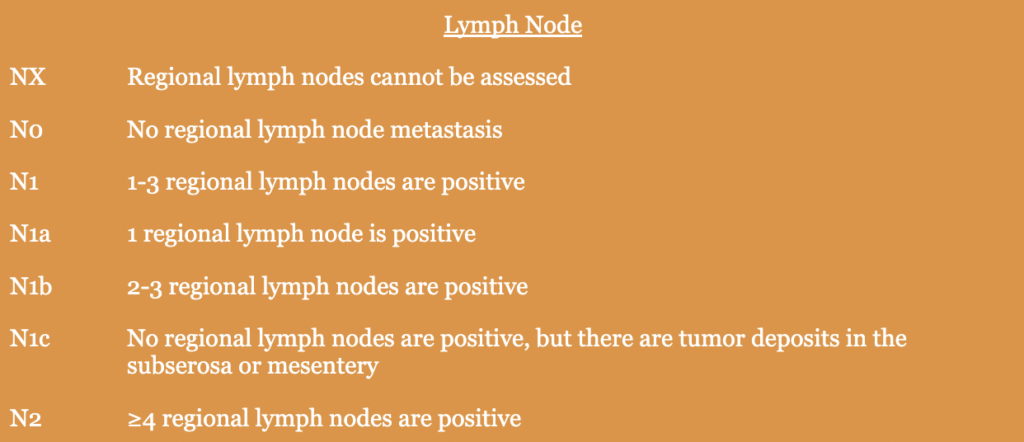
- Lymph node involvement
- Evidence of perforation
- Signet cell histology
- Poor differentiation
Relevant information
- 2% of all appendectomy specimens harbor an appendiceal neoplasm