Primary hyperparathyroidism occurs with the parathyroid glands secrete excess parathyroid hormone (PTH). Richard Owen was the first to describe the parathyroid gland after performing a postmortem exam of an Indian rhinoceros in London Zoo in 1852. The term “hyperparathyroidism” was coined by Henry Dixon and colleagues. Prior to this, Friedrich von Recklinghausen described osteitis fibrosa cystica in 1891.
Etiology
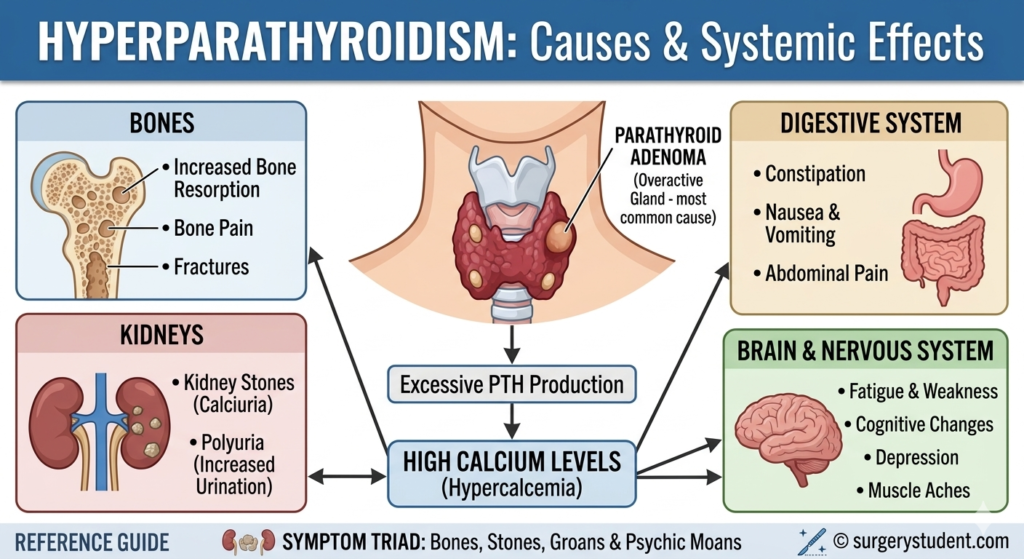
- Most common cause in outpatient setting → PHPT
- Single benign adenoma or hyperplasia (most common, 85%)
- Parathyroid carcinoma (1%)
- Risk factors:
Epidemiology
- Female predominance
- Older age
Pathogenesis
- Occurs when ≥1 parathyroid glands secretes excess PTH, if >1 gland is involved it is referred to as multigland disease
- Primary function is calcium homeostasis by secreting PTH
- Target tissues of PTH
- Bone → maturation of osteoclasts from progenitor cells leading to increased bone destruction and more calcium into blood
- Kidney → calcium reabsorbed in proximal and distal tubule
- Intestine → increase calcium absorption from intestine by increasing calcitriol (active form of vitamin D) which activates calcium-binding proteins to allow calcium to enter bloodstream
Presentation
- Most patients don’t have symptoms
- Frequent urination
- Poor sleep
- Difficulty with memory/concentration
- Anxiety, depression
- Fatigue, brain fog
- Constipation
- GERD
- Pancreatitis
- Kidney stones
- Severe bone loss → osteoporosis, bone pain, pathologic fractures
- End-stage renal failure
- Osteitis fibrosa cystica → brown tumors from calcium resorption
Workup
- Labs
- Total serum calcium: elevated, >14 mg/dL (ideally fasting)
- PTH: elevated or normal, >5 x upper limit of normal (ideally fasting) (if decreased, it is non-PHPT cause)
- 25-OH vitamin D: decreased
- Urine
- Calcium-to-creatinine ratio >0.02
- Rules out familial hypercalcemic hypocalciuria
- Dual-energy X-ray absorptiometry (DXA)
- KUB is ordered in patients with history of kidney stones
Imaging
- Imperative to decide, arrange, and review imaging once deciding to operate
- High-resolution ultrasound
- Recommended in all patients with PHPT who are planned for surgery as it helps with localization and deciding between partial or total thyroidectomy at the time of parathyroidectomy
- Assesses size, location, malignant potential of nodules
- Parathyroid scintigraphy (sestamibi) with or without SPECT
- Normal parathyroids are too small to be visualized
- Negative scan correlates with small gland size, coexisting thyroid disease, superior location, use of calcium-channel blockers, and MGD
- 4D-CT
- Higher radiation
- Often used when other localization studies are discordant or negative
Treatment
- Calcium-lowering medications (e.g., Cinacalcet)
- Surgery → parathyroidectomy
- Parathyroidectomy is the only curative treatment. The goal is to remove all hyperfunctioning tissue while preserving normal in situ parathyroids. Patients often demonstrate improvements in bone mineral density, fracture-free survival, renal dysfunction, nephrolithiasis, sleep, quality of life, neurocognitive function after surgery.
- Indications
- Symptomatic PHPT (e.g., osteoporosis, nephrolithiasis, neurocognitive debility, symptomatic hypercalcemia)
- Hypercalciuria >400 mg/24 hours
- Asymptomatic PHPT → developed by NIH in 1990
- Serum calcium level >1.0 mg/dL above upper limit of normal
- DXA T-score < -2.5
- Creatinine clearance <60 mL/min
- Urine calcium >400 mg/24 hours
- Nephrolithiasis
- Age <50
- Inability to comply with medical surveillance
- Approach
- Adenoma → focused parathyroidectomy (FP)
- Hyperplasia or MEN I/IIa → bilateral exploration (BE)
- 1-3 enlarged glands → resect all diseased glands
- 4 enlarged glands → subtotal (3.5 gland) resection or total parathyroidectomy with autoimplantation
- Adenocarcinoma → radical parathyroidectomy (no need for lymph node dissection)
Relevant Information
- Anatomy
- Superior parathyroids
- 4th pharyngeal pouch
- Associated with thyroid complex
- Commonly lie lateral and deep to recurrent laryngeal nerve
- Above inferior thyroid artery
- Inferior parathyroids
- 3rd pharyngeal pouch
- Associated with thymus
- More variable location than superior – usually lie medial and anterior (ventral) to recurrent laryngeal nerve
- Below inferior thyroid artery
- Inferior thyroid artery supplies blood to both superior and inferior parathyroid glands and approaches from a medial direction under the thyroid
- Superior parathyroids
- Intraoperative PTH during parathyroidectomy
- Detects immediate drop in PTH after resection of hyperfunctioning gland (using PIV, as it is more accurate)
- Miami Criterion
- Requires >50% drop in PTH after gland removal compared to preincision or pre-excision level
- If level doesn’t drop sufficiently after removing a single enlarged gland, then the patient likely has MGD and conversion to BE is appropriate
Differential Diagnoses
- Familial hypocalciuric hypercalcemia (FHH)
- Autosomal dominant
- Loss-of-function mutations in calcium-sensing receptor (CASR) gene
- Labs that should prompt further evaluation of FHH
- 24-hour urine calcium excretion <100 mg/24 hours
- Urinary calcium-to-creatinine clearance ratio <0.01
- Generally asymptomatic, nonmorbid condition
- Familial PHPT
- Sporadic disease
- Most cases are associated with MEN types 1 and 2A