
Necrotizing soft tissue infections (NSTIs) is a broad term used for infections in the skin and soft tissue. Hippocrates described these infections as early as the 5th century BC. The terminology surrounding NSTIs has changed throughout history. Dr. Ben Wilson coined the term “necrotizing fasciitis” in 1962 when he published a review of a case of a soft tissue infection in the American Surgeon.
Etiology
- Necrotizing soft tissue infection (NSTI): necrotizing infection of skin and soft tissue
- Necrotizing cellulitis: NSTI of skin
- Necrotizing fasciitis: NSTI of fascia
- Necrotizing myositis: NSTI to deep muscle compartments
- Fournier gangrene: NSTI of perineum
- Risk factors
- Skin trauma
- Skin inflammation
- Diabetes
- Immunosuppression
- Edema
- IV drug use
Presentation
- Crepitus
- Severe pain extending beyond the involved skin
- Late signs → bullae, blisters, fever, hypotension
Diagnosis
- LRINEC cannot be used as sole diagnostic tool
- Components
- Elevated WBC and CRP
- Hyponatremia
- Elevated creatinine
- Hyperglycemia
- Scoring
- ≤5 (low-risk) → 50% probability of NSTI
- 6-7 (intermediate-risk) → 50-75% probability of NSTI
- ≥8 (high-risk → >75% probability of NSTI
- Components
- CT scan → fascial gas
- Sensitivity: 88.5%
- Specificity: 93.3%
- MRI: higher sensitivity compared to CT
- Surgical exploration → gold standard for diagnosis
Treatment
- Emergency surgical exploration and debridement
- Preferably within 12 hours due to rate of progression
- Note: can progress to lethal infection within 24 hours
- Contraindications
- Patient refusal
- Difficult airway
- Respiratory failure
- Clinical instability
- Inability to tolerate surgery
- Intraoperative approach
- Wide debridement of all necrotic tissue
- Explore all areas with concerning skin changes (e.g., cellulitis, edema, petechiae, purpura, blistering)
- Obtain wound cultures
- Blunt finger dissection can expose additional areas of necrosis
- Likely require multiple debridements
- Findings
- Dishwasher fluid
- Tissues that are grey, pasty, and devitalized
- Vessel thrombosis
- Muscle that is nonreactive with electrocautery
- Absence of resistance with sliding finger against fascial planes
- Postoperative care
- Dressings should allow for frequent assessment (wet to dry dressings soaked in saline or Dakin solution)
- Multiple debridements
- Second-look should take place 12-24 hours after initial
- Hemodynamic instability and increasing pressor requirement should signal a need for additional debridement
- Options for definitive closure
- Skin grafting ± dermal matrix (i.e., NovoSorb Biodegradale Temporizing Matrix or Integra wound matrix)
- Flap closure
- Broad-spectrum antibiotics
- Coverage for Gram-negative, Gram-positive, and anaerobic bacteria
- Carbapenem (Piperacillin-Tazobactam) + MRSA-specific (Vancomycin) + Clindamycin
- Obtain blood cultures
Relevant Information
- LRINEC score
- Components: CRP, WBC, Hb, Na, Cr, Glucose
- Sensitivity 80%, specificity 67%
- Published in 2004 in Critical Care Medicine by Dr. Chong-Hao Wong
- Mortality: 5-25%
- Risk factors for increased mortality
- Age >50
- HR >110
- Body temperature < 36.8ºC
- WBC >40
- Cr >1.5
- BMI <18.5
- Sepsis at admission
- Dialysis
- Cancer diagnosis
- MRSA-specific antibiotic use
- Risk factors for increased mortality
Complications
- Multiple system organ failure
- Bleeding
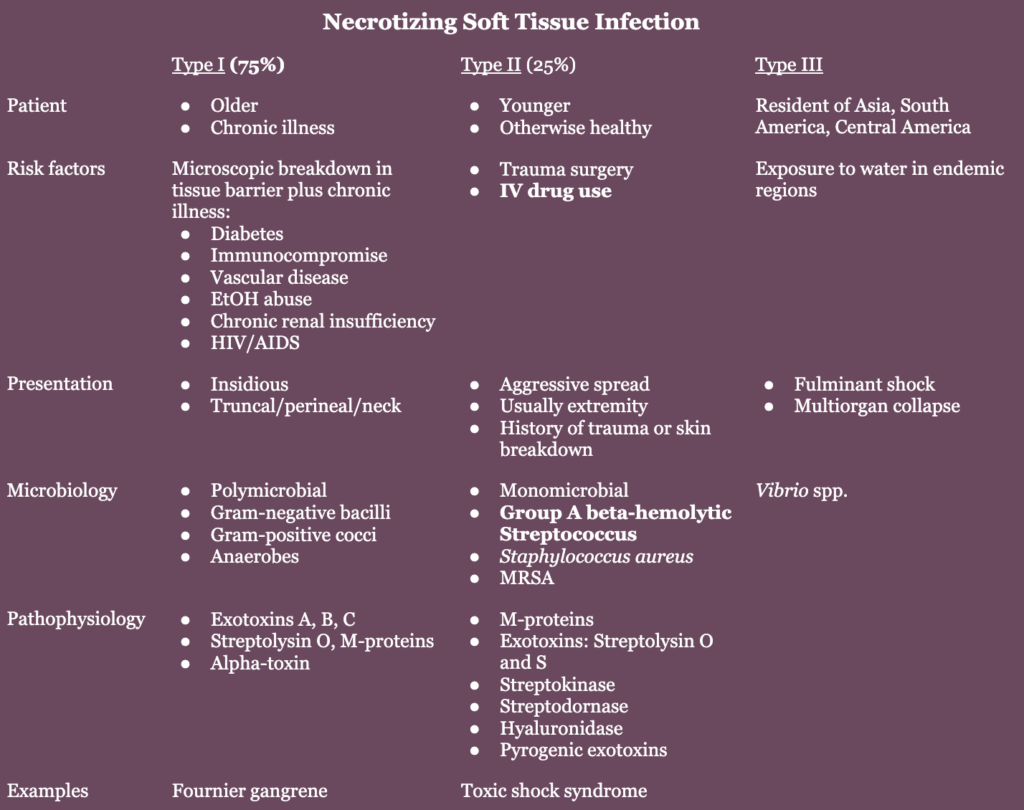
Types
Resources
- LRINEC score
- The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. (2004)