
Gastric and duodenal perforations occur for multiple reasons, as highlighted below. The first recorded perforated peptic ulcer was that of Princess Henrietta Ann, daughter of King Charles I of England. In 1880, the first attempt to operate on a perforated ulcer was performed by Mikulicz. It wasn’t until 1892 that surgery was successful – the operation included a primary repair with two silk sutures.
Etiology
- Peptic ulcer disease (most common)
- Helicobacter pylori
- Accounts for 70-90% of duodenal ulcers
- Accounts for 30-40% of gastric ulcers
- Potentiators
- Smoking
- Chronic alcohol consumption
- Zollinger-Ellison syndrome
- Renal failure
- Liver failure
- Helicobacter pylori
- Iatrogenic
- Trauma
- Malignancy → gastric cancer is most common primary to result in perforation
- NSAIDs
- Reduced prostaglandin production
- Impairment of barrier properties of mucosa
- Reduction in perfusion of gastric mucosa
Epidemiology
- Mortality 25%
- Age 40-50
Presentation
- Sudden-onset severe, unrelenting abdominal pain
- Gnawing, burning pain
- Febrile, diaphoretic
- Tachycardia
- Anxious
- Peritonitis
- Rigid, distended abdomen with rebound tenderness
Workup
- Gastrin levels >1000 pg/mL are suggestive of gastrinoma
- CXR: acute perforation with air under diaphragm
- CT A/P
- Diagnostic accuracy is 98%
- Flecks of extraluminal gas
- Upper GI
- Radio-opaque water-soluble contrast ingested to evaluate for extravasation under fluoroscopy
Preoperative Considerations in Duodenal Perforations
- Patient history of H. pylori and respective medical treatment is important to understand prior to progressing to the OR
- Patients who perforated despite being on antibiotics for H. pylori require different planning compared to those who developed duodenal perforations without prior diagnosis and treatment of H. pylori
Management
- Hemodynamic stabilization
- Guided by Surviving Sepsis recommendations
- Target MAP ≥65 mmHg
- Urine output ≥0.5 mL/kg/hr
- Lactate normalization
- Early initiation of broad-spectrum antibiotics
- Third-generation cephalosporin and metronidazole
- Monotherapy with beta-lactam/beta-lactamase inhibitor (e.g., piperacillin-tazobactam)
- Little benefit has been demonstrated for starting empiric anti-fungal coverage
- Control of spillage and placement of nasogastric tube
- IV proton pump inhibitors
- Expeditious definitive management
- Surgery is indicated in almost all cases
- Trial of nonoperative management can be attempted in patients who are asymptomatic, localized pain, clear contained perforation, or those unfit for surgery. This includes nasogastric decompression, broad-spectrum antibiotics, IV proton pump inhibitors, and percutaneous drainage of any intra-abdominal fluid collections.
- Surgery
- Source control. Suctioning and copious irrigation with warmed saline (>2-3L) to evacuate spilled gastric contents, succus, and fibrin.
- Biopsy. Should be performed on all spontaneous gastric perforations as there is high risk of malignancy (~5%). Obtain biopsy with Metzenbaum scissors to excise 5-10 mm of perforated tissue with care to include all layers of gastric wall. Note – duodenal perforations don’t require biopsy since ~90% are due to H. pylori.
- Gastric repair techniques
- Primary repair.
- Indications: traumatic or iatrogenic causes
- Inspect anterior and posterior gastric walls and gastroesophageal junction for additional injuries. Open gastrocolic ligament and inspect posterior gastric wall and pancreas. Debride nonviable tissue around the defect and close with full-thickness interrupted or running suture followed by a second layer of interrupted serosal Lembert sutures.
- Leave a drain
- Graham patch.
- Indications: small (<1 cm) gastric perforations
- Debride edges of gastric defect and obtain biopsy. Lay 2-0 silk sutures across the defect by grabbing 5 mm full-thickness bites of healthy gastric tissue on each side, leaving edges of each suture long and untied. Obtain a tension-free, well-vascularized portion of [free] omentum and lay it over the perforation then tie the sutures to anchor the omental graft in place.
- Leak test is not recommended. Leave nasogastric tube in place and is generally safe to remove and start diet without a study to investigate the repair in 48-72 hours.
- Modified Cellan-Jones.
- Indications: same as Graham patch repairs
- Debride edges of gastric defect and obtain biopsy. Lay 2-0 silk sutures across the defect by grabbing 5 mm full-thickness bites of healthy gastric tissue on each side and tie them down, leaving edges of each suture long and tied. Obtain a tension-free, well-vascularized portion of [pedicle] omentum and lay it over the perforation then tie the long tails of the suture down again to anchor the omental graft in place.
- Modified Graham patch.
- Indications: small (<1 cm) gastric perforations
- Debride edges of gastric defect and obtain biopsy. Lay 2-0 silk sutures across the defect by grabbing 5 mm full-thickness bites of healthy gastric tissue on each side and tie them down, leaving edges of each suture long and tied. Obtain a tension-free, well-vascularized portion of [free] omentum and lay it over the perforation then tie the long tails of the suture down again to anchor the omental graft in place.
- Leak test is not recommended. Leave the nasogastric tube in place and is generally safe to remove and start a diet without a study to investigate the repair in 48-72 hours.
- Pedicled omental plug.
- Indications: larger (>2 cm) perforation
- Tongue of well-vascularized omentum is created. Nasogastric tube is placed and passed out through the gastric perforation. Omental plug is loosely tied to the end of the nasogastric tube with absorbable chromic suture. Nasogastric tube is slowly withdrawn until the plug snugly fills the perforation and the tube is taped down at that location.
- The tube is left for a minimum of 4 weeks. At this point, suture has had breakdown and can be removed without resistance. If resistance is felt, the tube should be left longer.
- Gastric resection and reconstruction.
- Indications: perforations not amenable to patching, recurrent perforations
- Wedge resection.
- Indications: perforations along greater curvature
- Clear omentum from greater curvature. Linear stapler used to excise perforated tissue and adjacent segment of gastroepiploic artery in “V”-shaped fashion. Healthy tissue margins 5-10 mm around perforations should be obtained to ensure all nonviable tissue is excised and that adequate biopsy is obtained.
- Antrectomy and reconstruction.
- Indications: perforations along lesser curvature, refractory PUD
- Primary repair.
- Duodenal repair techniques
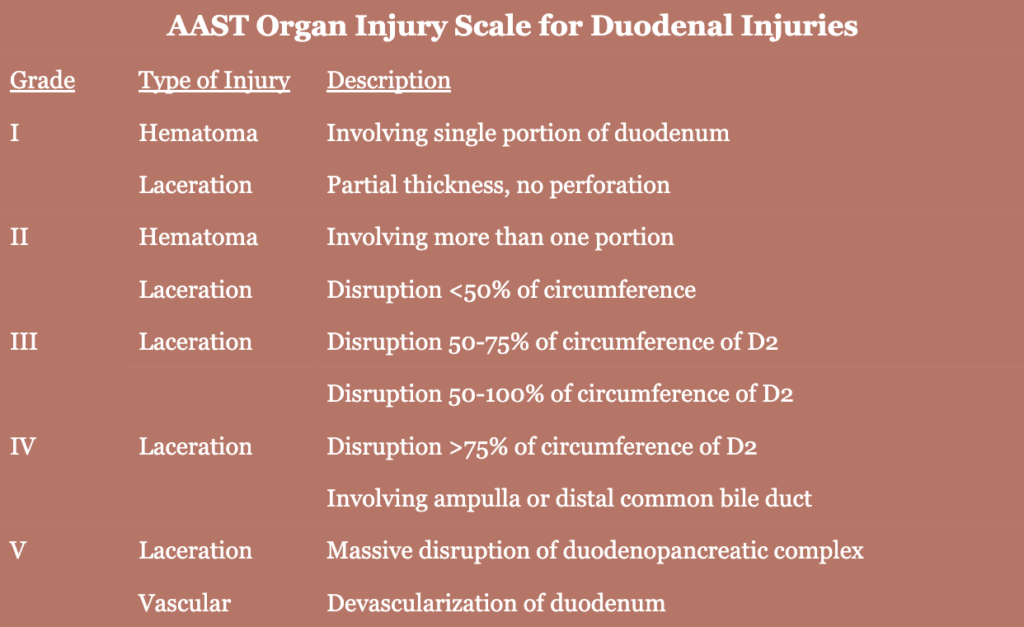
- Grade 1 and 2 perforations → local repair
- Grade 3 and higher perforations → complex resection and/or reconstruction
- Primary closure.
- Minimal debridement of wound margins as needed
- Close linear lacerations transversely to avoid luminal narrowing
- Closure with running or interrupted sutures either in one or two layers as dictated by local conditions
- Care must be taken to ensure ampulla isn’t involved in the perforation closure
- Nasogastric placement prior to primary closure
- Omentum patch and plug techniques.
- Graham patch
- Primary closure of perforation followed by covering repair with omental flap as patch or buttress and secure omentum with interrupted suture circumferentially
- Jejunal serosal patch.
- Jejunal loop is brought up and placed adjacent to perforation and secured with either running or multiple interrupted sutures using full-thickness bites of perforation margin to seromuscular bites of jejunal patch.
- Significant failure rate for bigger defects
- Duodenojejunostomy.
- Jejunal loop is brought up and placed adjacent to perforation and a matching enterotomy is made on the antimesenteric border of jejunum. Handsewn side-to-side anastomosis is made using slowly absorbable sutures in a running fashion.
- Allows for wide outflow and duodenal perforation.
- Duodenal resection.
- Tube duodenostomy/jejunostomy.
- Pyloric exclusion.
Postoperative Management
- Continue nasogastric or orogastric decompression
- Exact length of time varies
- Output >1000 mL/24 hours indicates need for continued decompression
- <500 mL bilious output is indicator for discontinuation
- Little data to support routine contrast imaging prior to NG tube removal and initiation of enteral intake
- Simple repairs → PO liquids initiated 24-48 hours after surgery and advance as tolerated
- Complex disease → enteral nutrition via nasoenteric or surgical feeding tube distal to injury site within 48-72 hours
- Strong evidence that there is no benefit to perioperative antibiotics beyond 24 hours after surgery
Postoperative Complications
- Surgical site infections
- Diagnosed with CT A/P when clinically suspected
- Manage with image-guided percutaneous drainage or antibiotics and repeat imaging if small (≤2-4 cm) abscess
- Leak from repair or anastomosis
- Risks: larger perforation, duodenal location, complex reconstruction
- Management
- Wide local drainage
- POD 5-7 → abdominal exploration
- POD ≥8 → surgical or image-guided drain, hold enteral nutrition
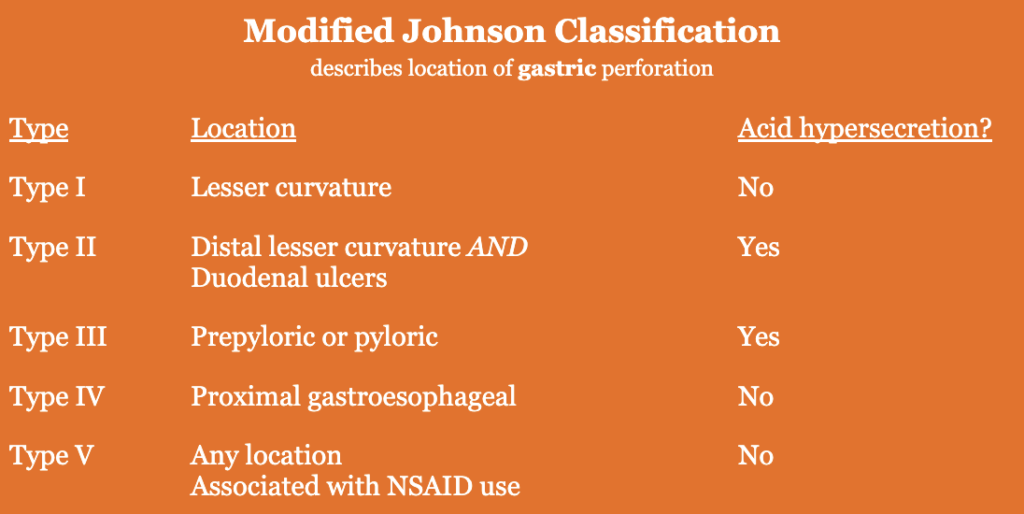
Classifications
Resources
- Management of Perforated Peptic Ulcer: A Review (JAMA 2025)
- Perforated and Bleeding Peptic Ulcer Guidelines (WSES 2020)