
In 1879, Jules Emile Pean performed the first gastric resection for cancer. The first partial gastrectomy occurred in 1881 and was by Theodor Billroth.
Etiology
- Genetic syndromes
- Hereditary diffuse gastric cancer
- Lynch syndrome
- Familial adenomatous polyposis
- MUTYH-associated polyposis
- Peutz-Jeghers syndrome
- Li-Fraumeni syndrome
- Risk factors
- H. pylori (most common)
- Smoked meats, pickled foods, high sodium
- Tobacco
- Blood type A
- Chronic gastritis and pernicious anemia
- Epstein-Barr virus
Pathogenesis
- Four genomic subtypes
- EBV-infected tumors
- Microsatellite unstable (MSI-high) tumors
- Genomically stable tumors
- Chromosomally unstable tumors
Presentation
- Nonspecific
- Abdominal pain
- Nausea, vomiting
- Anorexia
- Dyspepsia
- Acid reflux
- Fatigue
- Weight loss
- Anemia
- GI bleeding
- Metastatic disease
- Cachexia
- Jaundice
- Ascites
- Hepatomegaly
- Classic symptoms (that are rarely present) → advanced metastatic disease
- Virchow’s node
- Sister Mary Joseph’s periumbilical node
- Blumer’s shelf
Workup
- Flexible upper endoscopy
- Establishes the diagnosis most easily
- More costly
- Localizes primary tumor
- Can biopsy during evaluation
- Benign ulcers: round/oval shape with smooth rim that projects beyond lumen
- Malignant ulcers: irregular shape with associated mass that projects inside lumen
- More sensitive and specific for gastric cancer than any radiographic study
- Double contrast upper GI
- May be better to diagnose linitis plastica than flexible upper endoscopy
- Biopsy
- Sensitivity 70% (single biopsy)
- Sensitivity 98% (seven biopsies)
Staging
- Physical exam
- Lab studies
- H. pylori status
- Endoscopy with EUS staging and biopsy
- More accurate to evaluate T stage
- Recommended in treatment guideline as part of pretreatment staging of gastric cancer in patients who have no evidence of metastatic disease
- CT C/A/P ± PET
- CT evaluates for distant metastasis to lungs, liver, peritoneum, or lymph nodes
- CT is less accurate in T stage is 60%
- Resectable → T1 tumor → resection with EMR or partial gastrectomy
- T2-4 or N+ tumors → laparoscopy with cytology ± J-tube
- Diagnostic laparoscopy
- Skip if T1a
- Stage ≥T1b prior to gastrectomy or perioperative chemoradiation
- Prior to preoperative chemotherapy
- Presence of GE-junction tumor or tumor involving entire stomach
- Lymphadenopathy ≥1 cm
Treatment
- Immediate resection
- Indications
- Early stage (T1/T2 N0) gastric cancers
- Immediate palliation of bleeding
- High-grade tumor-associated luminal obstruction
- Should undergo adjuvant chemotherapy if T3/T4 and/or node-positive
- Indications
- Staging laparoscopy
- All gastric cancers of clinical tumor stage T2 or greater
- Peritoneal carcinomatosis is a common pattern of metastasis and CT scans have a low sensitivity for detecting this
- Peritoneal washings for cytology should be obtained
- Locoregionally advanced gastric cancers → perioperative chemotherapy with four cycles of FLOT (5-FU, leucovorin, oxaliplatin, docetaxel) delivered before and after surgery
- Resectable gastric cancer
- Approach
- T1a (superficially invasive) → endoscopic mucosal resection or wedge excision +/- SLNB
- Proximal tumor → total gastrectomy (reconstruct with Roux-en-Y)
- Distal tumor → distal gastrectomy (reconstruct with Roux-en-Y or Billroth II)
- Margins: 4-6 cm
- Residual disease
- R0 → no residual disease
- R1 → microscopic residual disease
- R2 → gross residual disease
- Lymph node dissection
- D1: perigastric nodes (stations 1-6)
- D2: common hepatic, left gastric, celiac, and splenic arteries (stations 7-11; generally recommended)
- D3: porta hepatis nodes and those adjacent to aorta (stations 12-16; no survival benefit)
- Approach
- Chemotherapy
- Neoadjuvant: ≥T2 or N1
- Adjuvant: ≥T3 or N1
Relevant Information
- Metastases
- Sister Mary Joseph nodule: metastasis to umbilicus – suggests carcinomatosis
- Krukenberg tumor: metastasis to ovary
- Virchow node: metastasis to supraclavicular node
- Irish nodule: metastasis to left axilla
- Complete, margin-negative (R0) resection is only potentially curative surgical option for gastric adenocarcinoma
- Per AJCC guidelines, accurate staging requires at least 16 lymph nodes in order to assess N stage
Lauren Classification
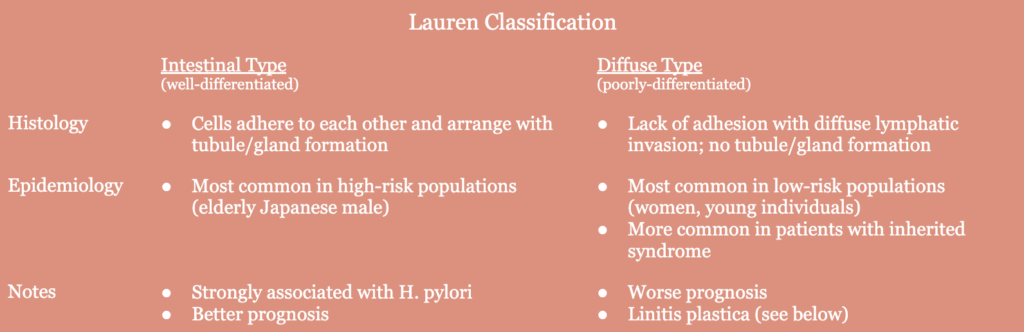
- Linitis plastica
- Diffuse-type gastric cancer
- Difficult to diagnose endoscopically as the tumors originate and spread in submucosa which can make the mucosa biopsies falsely negative
- Tumors originate and spread within submucosa
Resources
- Current management of gastric adenocarcinoma: A Narrative Review (Journal of Gastrointestinal Oncology – 2023)
- Stomach Cancer (American Cancer Society)